—written by H Chamdawala MD MPH & J Gombar MD
A 6 month old female presents with one day of vomiting and episodic back arching, associated with decreased oral intake and no bowel movement for the past two days. She has been afebrile. On examination, she appears tired and mildly dehydrated, and she cries during the abdominal examination, which limits full assessment. The differential diagnosis includes viral gastroenteritis, intussusception, and gastroesophageal reflux, among other causes of vomiting and abdominal discomfort in this age group.
Scanning technique: When evaluating for intussusception with point-of-care ultrasound (POCUS), the infant is placed supine and a high-frequency linear transducer is used initially, with a curvilinear probe available for deeper or larger fields of view. The abdomen is scanned systematically in transverse and longitudinal planes, starting in the right lower quadrant and sweeping through the right upper quadrant, epigastrium, and left abdomen, with particular attention to the periumbilical region and right upper quadrant, where intussusception is most commonly identified. Graded compression is applied to displace bowel gas and improve visualization. On POCUS, intussusception classically appears as a “target” or “donut” sign in the transverse view, characterized by concentric hypoechoic and hyperechoic rings, and as a “pseudokidney” or “sandwich” sign in the longitudinal view. Associated findings may include proximal bowel dilation, free fluid, or absent peristalsis within the involved segment.
Teaching points:
A systematic abdominal sweep is critical, as intussusception may be intermittent or migrate.
Graded compression improves sensitivity by reducing bowel gas.
A persistent, non-compressible target lesion is more concerning for pathologic intussusception.
Presence of free fluid or bowel wall edema may suggest a more advanced process and warrants urgent consultation.
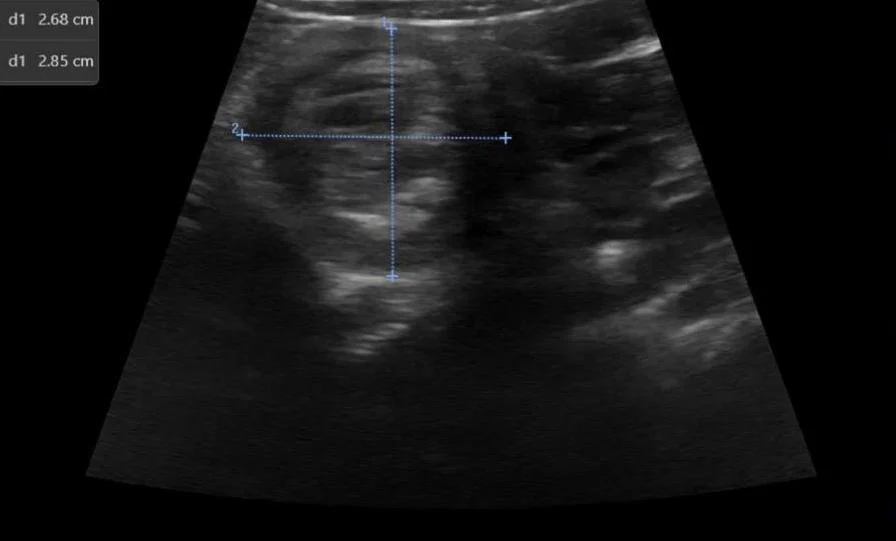
Image 1: Intussusception short axis diameter measurements.
Clip 1: Intussusception short axis.
Clip 2: Intussusception long axis.
Clip 3: Intussusception long axis.
Clip 4: Intussusception short axis.
Clip 5: Intussusception short axis.